

PROJECT FOUNDATIONS
PRADA was coordinated by a small leadership team that included ACP staff, a member of the iConquerMS RIDE Council, and an independent professional facilitator. This team supported the process administratively and logistically, while research priorities and decisions were driven by community input.
A multi-stakeholder steering committee was convened in October 2024 to guide the project. The committee included iConquerMS community members, RIDE Council representatives, researchers, clinicians, and a representative from the National MS Society. Early meetings focused on shared goals, timelines, and guardrails to keep the process community-centered.
GATHERING COMMUNITY PRIORITIES
PRADA is built on the Our Questions Have Power program, which invites iConquerMS members to submit topics related to MS symptoms and treatments they want the research community to address. Prior to PRADA’s launch, approximately 40 questions related to MS symptoms and their treatment and management had already been submitted.
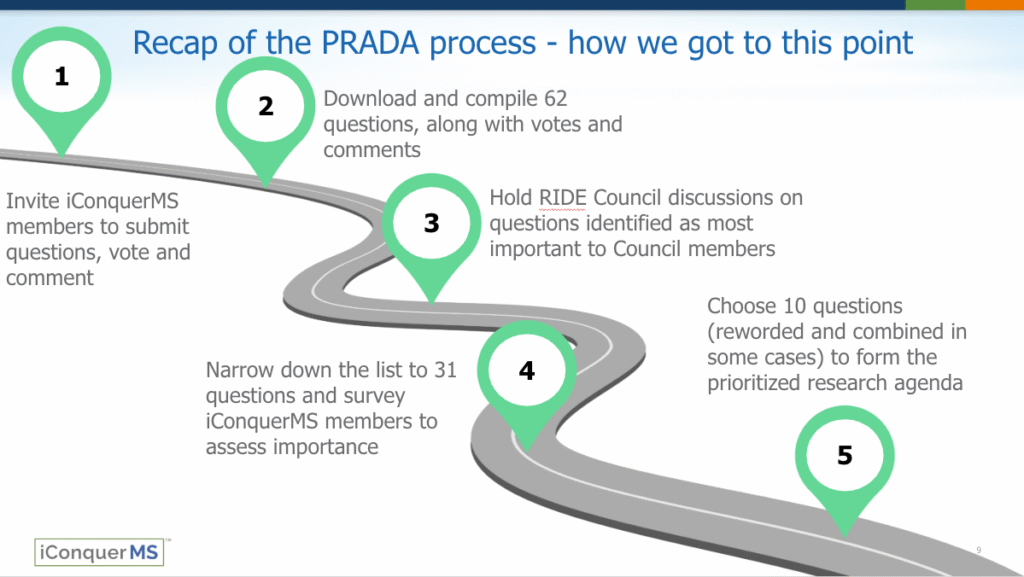
With the launch of PRADA, iConquerMS members were invited to propose additional questions and to vote and comment on existing ones. In total, 62 research questions were submitted by community members. These questions and associated engagement data formed the foundation for the prioritization process.
CENTERING UNDERREPRESENTED VOICES
Members of the iConquerMS RIDE Council reviewed the full set of submitted questions and independently selected their top priorities. To avoid bias, Council members were not shown overall community voting results.
RIDE Council sub-councils—including Black/African American, Hispanic/Latinx, and Emerging Voices groups—met separately in facilitated discussions to explore which questions mattered most and why.
![]() These conversations focused on unmet needs, community concerns, and the real-world impact of MS, and the insights were documented and incorporated into later decision-making.
These conversations focused on unmet needs, community concerns, and the real-world impact of MS, and the insights were documented and incorporated into later decision-making.
REFINEMENT AND BROADER VALIDATION
After incorporating RIDE Council input, the Steering Committee reconvened to review both community engagement data and qualitative feedback. From the original 62 questions, the committee identified 31 priority questions that reflected shared importance across both the broader iConquerMS community and RIDE Council members. Minor wording changes were made to improve clarity and inclusivity.
These 31 questions were then redistributed to the broader iConquerMS community through an online survey. More than 600 members rated the importance of each question on a 1-5 scale and provided demographic information to help interpret the results and surface priorities across different communities.
FINALIZING THE PRADA AGENDA
The Steering Committee met again to review survey results, paying close attention to how questions were rated across demographic groups. Special consideration was given to feedback from historically underrepresented communities to ensure the final agenda reflected diverse perspectives.
Based on this review, ten research questions were selected, with final wording refined once more as needed for clarity and inclusivity. A brief literature scan was conducted to understand existing research related to each topic and identify evidence gaps, and the committee confirmed the final list.
MOVING FORWARD
The PRADA project has produced a people-powered research agenda shaped directly by the community it is intended to serve. These priorities are now being shared with researchers, funders, and partners to help inform study design, funding decisions, and future MS research efforts.
PRADA demonstrates what is possible when people affected by MS are not only consulted—but invited to lead in setting the research agenda.